
You are on your way to participate in a humanitarian mission.When you get there, you witness the outbreak of intense fighting which results in mass casualties at the scene.
Your task is to spot the people who should get medical care.
We have saved patients and are waiting for you to be a part of the mission!




On the next page, please click on all the patients you think should get medical assistance
so that they can be treated immediately.
 Time limit: 20 seconds
Time limit: 20 seconds




Providing treatment to malnourished children, assisting mothers to give birth, treating patients in an epidemic…These are perhaps the impressions you have of Médecins Sans Frontières / Doctors Without Borders (MSF). Apart from meeting these very visible needs, a large part of MSF’s work focuses on providing care in hidden emergencies, which, while receiving little media coverage, can be just as serious.
In every situation, MSF strives to ensure that we target people who may be overlooked by the authorities or by other aid groups. These neglected populations may include sex workers, prisoners, drug addicts, street children, or the mentally ill. Or in some places, when entire populations are systematically neglected by the authorities for ethnic or political reasons, MSF can step in to provide medical assistance to these people.
MSF sees only the medical needs of an individual, irrespective of their background, and provides treatment to meet those. Their race, religion, gender or political affiliation is not a factor.


In some countries, prisoners may have little or no access to health care.
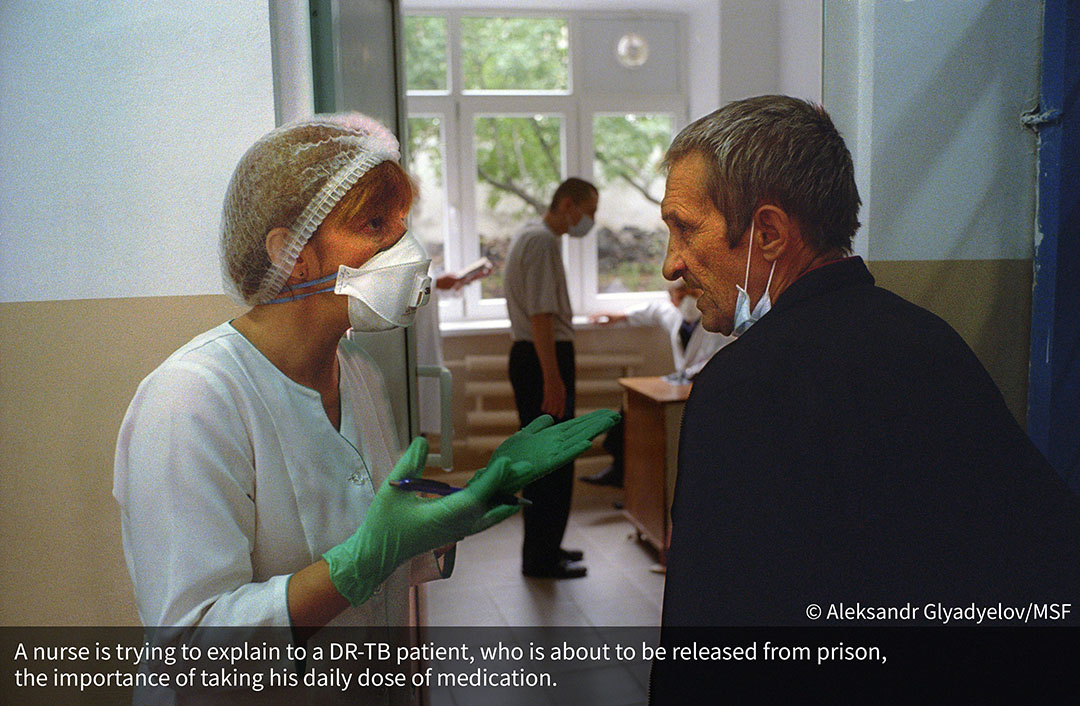
MSF has worked in Maula and Chichiri central prisons in Malawi since 2014. Overcrowding is a critical problem. One of the most crowded cells have the most case of disease transmission (Tuberculosis, Hepatitus, Malaria and HIV) as well as a high percentage of other diseases related to unhygienic conditions (scabies, skin infections, rash etc.).
Nutrition is another major concern. The Malawian Government allocates a limited budget to the penal system. And most of the prisoners eat only once a day.
Amongst this desperate population, the most vulnerable are the undocumented migrants. Most of them are Ethiopians who tried to go to South Africa for better paid work. When they are caught, they go to jail for three months. But then they are stuck because they have to pay for their own repatriation back to Ethiopia.
MSF is providing therapeutic food supplements to severe and moderately malnourished inmates and basic health care for prisoners as well as staff. We are also trying to treat a neglected group of prisoners who have HIV and TB.
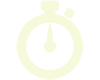
In Ukraine, the conditions in the prisons can sometimes speed the transmission of tuberculosis (TB), an already rampant disease in the country. The rate of TB is ten times higher in the prison system than in the rest of society.
Apart from supporting diagnosis and testing and providing medical treatment, MSF provides psychological support to TB patients to help them stay on treatment. Once the prisoners are released, MSF continues to provide medical and counselling support to the patients.






Sex workers have a high risk of contracting HIV but often find it harder to get antiretroviral care due to stigma and discrimination. Reaching this high risk group with treatment and advice that helps them stay safe is one of the keys to getting the epidemic under control.
Beira is a busy harbor city in Mozambique, the beginning and end of truckers’ routes distributing goods throughout Southern Africa. Mozambique’s mining boom has attracted migrant workers and sex workers from the neighbouring countries.
Many of the sex workers are trying to earn money to support their families. They have however very little protection from HIV. Even if they have condoms, it is sometimes difficult to convince the clients to wear them. “If a client insists to do it without, I sometimes have to accept as I need the money,” said Mary*, a Zimbabwean sex worker in Beira. This is one of the reasons why the virus is allowed to run free: 30% of the women surveyed by MSF who were HIV negative a year ago had contracted the virus within twelve months. Many Zimbabwean sex workers are especially reluctant to go to health centres because they are afraid they will be treated badly just because of what they do.
To increase access and improve adherence to treatment among this vulnerable group, MSF launched the “Corridor” project in 2014 to provide support and care to thousands of sex workers and the truck driver clients in the Beira corridor, which spans Mozambique, Malawi and Zimbabwe. Former sex workers are recruited as peer educators because they will be trusted most when they are advising about sexually-transmitted diseases and HIV.
*The name of the the sex worker has been changed for privacy concern.






Drug users are another vulnerable group of people who are often excluded from health care and treated very differently from the rest of the community.
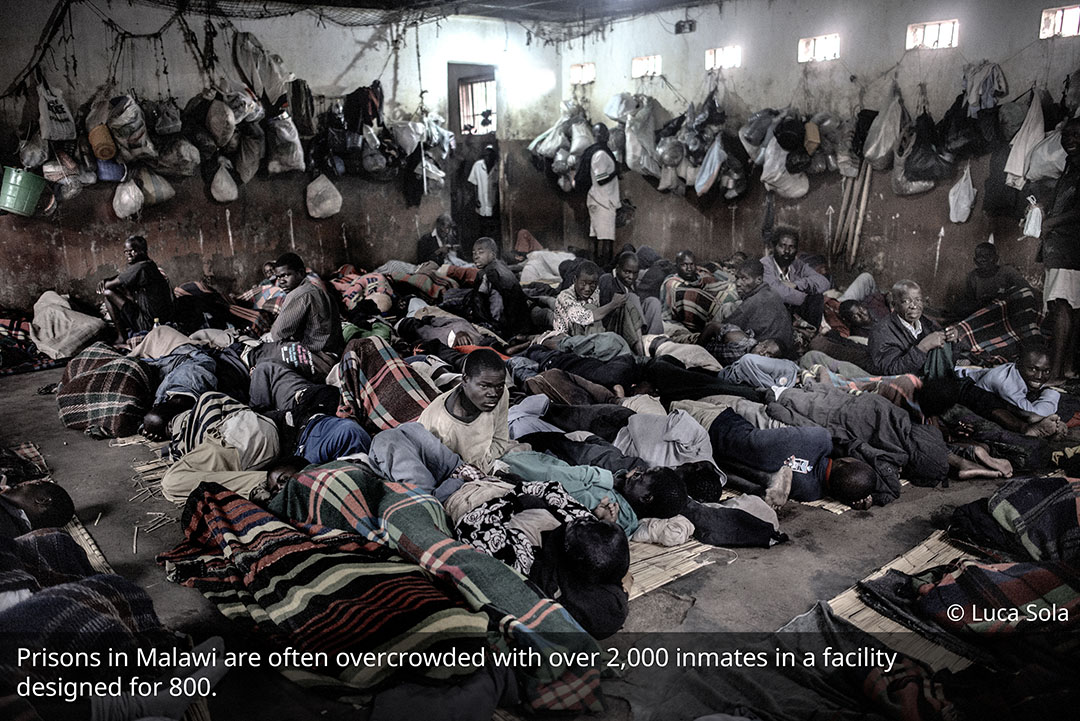
In Tehran, Iran, not everyone knows about Darvazeh Ghar. It is one of the Tehran’s poorest neighbourhoods south of the Grand Bazaar. Housing there is inexpensive but often poorly maintained. This is where people end up if they can’t afford to live anywhere else. There coexist daily workers, traders, street children, sex workers and drug users. Marginalised, destitute and sometimes without identity papers, these people have very limited access to basic health care.
MSF runs clinics for high-risk groups including sex workers and drug users in Darvazeh Ghar. “We treat refugees, ‘gypsies’ and pregnant, drug-addicted women. It’s hard for them to pay for their treatment and they can’t travel further to the Ministry of Health clinics,” said Mora, an MSF midwife who worked in the project in 2013. They are often marginalised and stigmatised and are afraid of being arrested. That prevents them from accessing “standard health services” provided by the government.
At the MSF clinic, these hard-to-reach groups can receive comprehensive healthcare, including general medical consultations, mental healthcare, reproductive and sexual health services, testing for HIV, TB, hepatitis C and other infectious diseases and vaccinations. Psychosocial support is also available. Health training is provided through group consultation for drug users, with the support of mental health team, including a psychologist, social worker and peer workers.




Migrants and refugees are not always welcomed. In some countries, they are put in detention centres as illegal aliens, and they won’t know when they can be released.
While migrants and refugees continue to leave the Libyan coast for Europe, they are constantly pushed back. European funding is paying for patrols to stop the boats from departing Libyan waters, in the hope of keeping people outside of Europe. But the result is that many are left in arbitrary detention in Libya. “Detainees are stripped of any human dignity, suffer ill treatment and lack access to medical care,” said Dr. Sibylle Sang, a medical advisor for MSF.
Overcrowding is one of the main causes of sickness in the detention centres. Medical teams treat more than a thousand detainees every month for respiratory tract infections, acute watery diarrhoea, infestations of scabies and lice, and urinary tract infections. These diseases are directly caused or aggravated by detention conditions. Many detention centres are dangerously overcrowded with the amount of space per detainee so limited that people are unable to stretch out at night and there is little natural light or ventilation. Food shortages is another problem. Sometimes detainees have gone for days at a time without any food at all.
Detainees also have to face torture. Most detainees are too afraid to speak about the violence and ill-treatment they suffer, but medical teams treat trauma-related injuries on a weekly basis and have treated detainees with broken legs and gunshot wounds. Men and women detained are also subjected to physical abuse, rape and extortion.







In conflict zones, MSF observes its principle of neutrality and does not take sides. We provide medical care based on needs alone, and work hard to try and reach the people who need help the most.
Anyone who is sick or wounded and arrives at our medical facilities would be just that, our patient, as long as they respect our policy and leave their weapons outside. Whether they are fighters or not, whichever side they are fighting for, they would receive the same treatments based on their medical needs.
A full-scale war has been raging in Yemen since March 2015. In April that year, our project coordinator in Aden at that time, Valérie Pierre, wrote about how the war brought scores of war-wounded to the surgical project where she was working. “It is not for us to ask how our patients were wounded – our business is only to provide medical care. Some of those who come to us for treatment will doubtless be fighters, but they respect our rules to leave the conflict at the door and know that we treat people from both sides.”
Another project coordinator who worked in Aden from May to August 2015, Thierry Goffeau, recalled that there were frequent nearby clashes between the Saudi-led coalition-supported Southern Resistance fighters and the Houthi rebels. “We managed to maintain the neutrality of this facility.” He continued, “We had Houthi and Southern Resistance wounded side by side. We were able to make sure that the Southern Resistance fighters did not touch the Houthi wounded, who were recognized as prisoners of war.”
MSF’s principles of impartiality and neutrality are also reflected in international humanitarian law (IHL), where medical personnel are obligated to treat all patients withoutdiscrimination. Patients are not registered according to their ethnicity, politics, religion, or participation in prior hostilities. They are triaged only according to their medical needs and the urgency with which they need to be seen. Withholding care or providing care in a discriminatory fashion is strictly prohibited.



While these groups of people come from different backgrounds and may not be highly regarded in their societies, MSF sees them differently. What we care about are their medical needs - MSF offers assistance to people based on need and irrespective of race, religion, gender or political affiliation.
The overall ethical principle here is about the responsibility of a doctor towards their patient, whoever they are , whether they are a good or bad person, whether you agree with their politics or their way of living, whether they have made choices that seem immoral or anti-social.
For MSF, the principles are about our shared humanity, about the fragility and vulnerability of each of us when we are sick or injured. Where those needs are desperately neglected or even denied, MSF will try to fill the gap.
So whether it’s the civilian, the boy on the top in the picture below, who was injured in the cross-fire, or the fighter on the bottom, both are patients first and last. We take no sides when saving lives.
If you support our humanitarian principles and work, please share the message with your friends. For latest news of MSF’s humanitarian work, please browse our website or like our Facebook Page.

